
This Case Report was published in GE Healthcare ASSIST Magazine, Issue 9, May 2021.
Patient History
A 62-year-old male patient was admitted for invalidating claudication of the left lower limb. He had pain with cramps in his calf with a walking distance limited to 50 m. Doppler ultrasound highlighted a short occlusion. CT angiography confirmed the same lesion with an external iliac lesion next to the hypogastric artery. An endovascular recanalization of the superficial femoral and popliteal arteries was proposed to the patient.
Clinical Challenge
The CTO of the superficial femoral artery was very calcified, leading to a high risk of dissection while crossing the lesion.
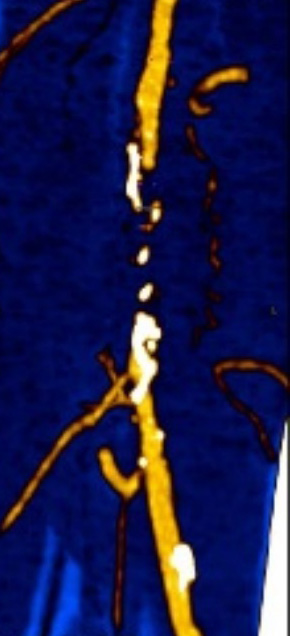
Fig 1. “Perfusion” mode on the preoperative CT. Calcifications are identified in white, in black we can identify the intima and in yellow the lumen of the vessel.
Procedure
Plan
It was possible to locate the calcifications on the preoperative CT, to identify their density and the lumen of the vessel thanks to the “perfusion” visualization mode.
Bone volume was automatically extracted thanks to Vessel ASSIST[1] and the centerline of the vessels was automatically tracked down to the occlusion, and manual tracking was performed at the level of the occlusion.
The calcification volume was extracted to be used as a landmark during guidance. Contour lines (circles) were planned at the level of the occlusion to give the best angulation for the recanalization during the guidance. Best angulation found was 24°RAO, 3°CAU. The patient was installed in a supine position on the Innova IGS 530 system. The procedure was performed under local anesthesia.
Guide
The volumes extracted from the pre-operative CT were fused with live fluoroscopy thanks to Vessel ASSIST. A registration was performed with the “Bi-View” mode based on the bone structures close to the area of the interest. Heparin was administered to the patient. Puncture of the right common femoral artery was performed under ultrasound guidance. A 5F introducer was used for the catheterization and a right-left crossover was performed with a dedicated probe.
Active balloon angioplasty and stenting of the popliteal artery
Once the catheter was placed at the level of the popliteal artery, the initial registration was finetuned based on the first arteriography. (Fig. 2)
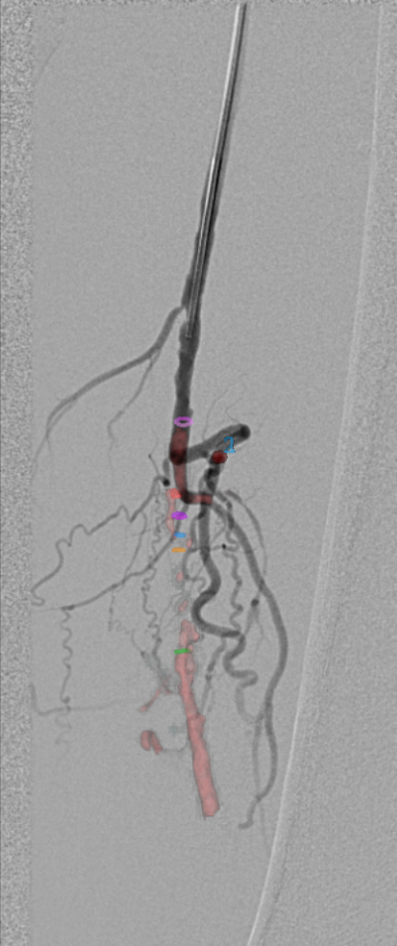
Fig 2. Fine tuning of the initial registration using DSA.
Digital zoom was used for a better visibility without changing the size of the field of view and thus without increasing the radiation dose. Vessels, calcification and contour lines were fused with live fluoroscopy. The 24°RAO, 3°CAU working incidence was automatically recalled from table side. A 0.18mm guide was used for the procedure. Collateral vessels seemed to interfere with the guide during catheterization and, relying on fusion imaging, the guidewire seemed to dissect the occluded vessel. (Fig. 3)
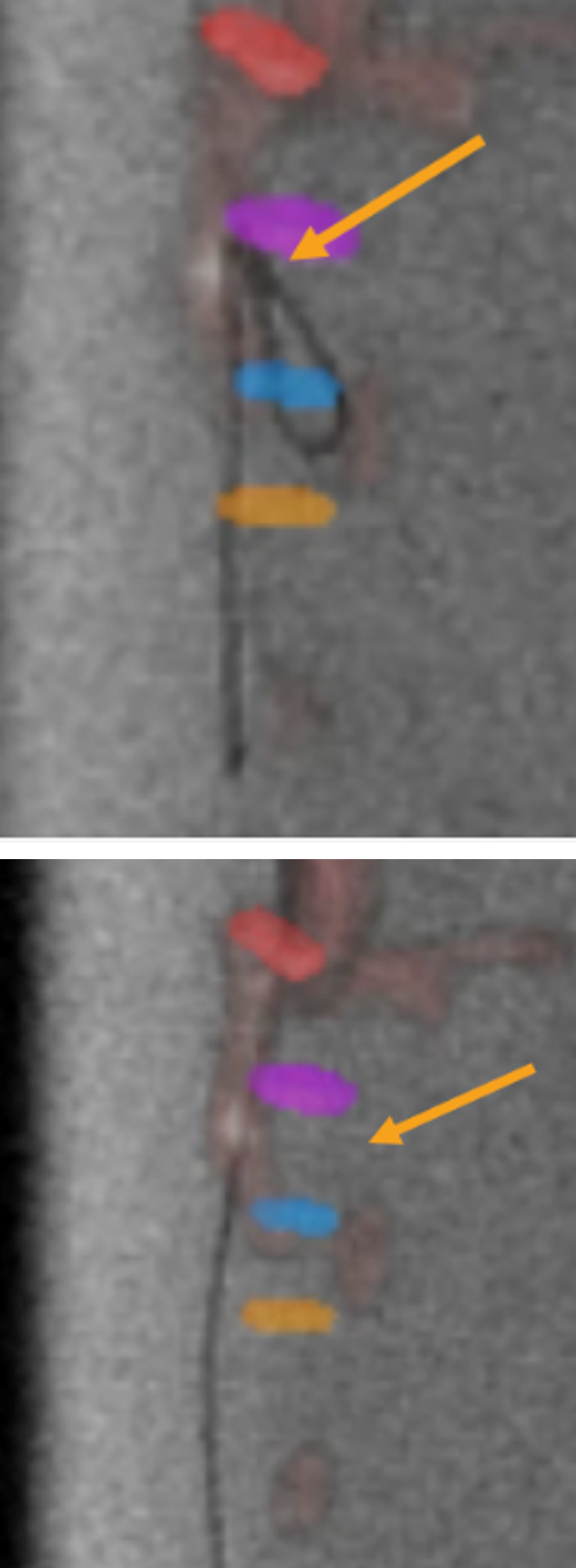
Fig 3. Guidewire navigation inside the occlusion, the guidewire seems to go outside of the vessel.
The guide was then re-positioned relying on the CT fusion. Initial catheter and guide were replaced with dedicated ones for an optimal crossing of the lesion. The probe was advanced through the lesion, and no dissection was observed while crossing the lesion, which avoided the use of a reentry system. (Fig. 4)
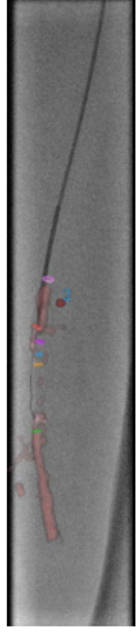
Fig 4a. Guidewire going in dissection.
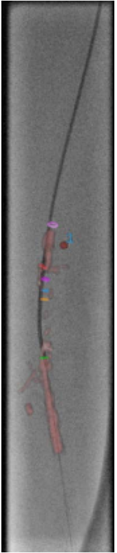
Fig 4b. Crossing the lesion using a dedicated catheter and guide.
A 4x60 balloon was used and inflated during 3 minutes. A 5x100 active balloon was then inflated for 2 minutes. A small proximal dissection was identified. A Supera7 5.5x60 stent (Abbott Vascular, USA) with the same size balloon was positioned. The results on the injected acquisition were very satisfying. (Fig. 5)
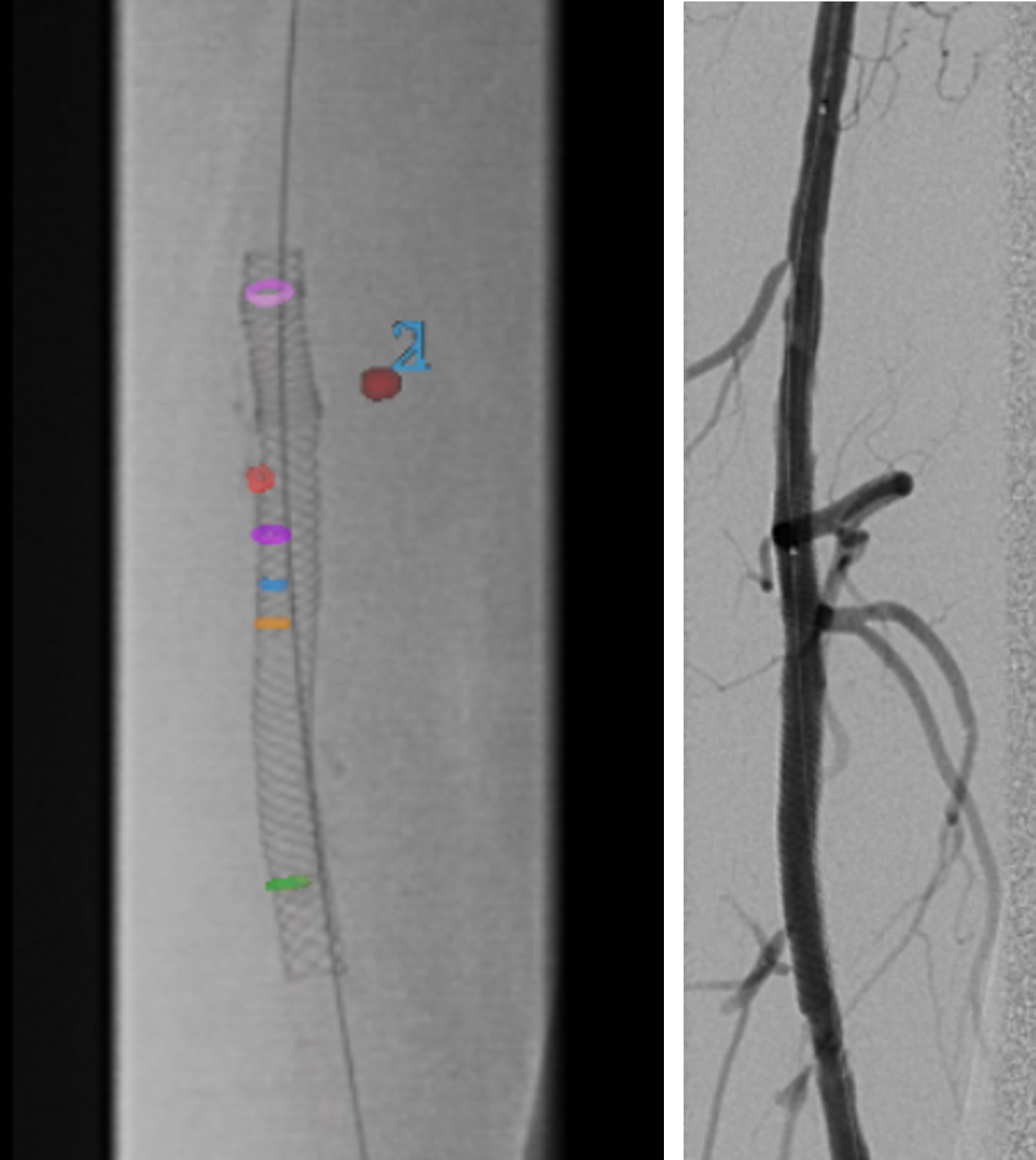
Fig 5. Fluoroscopy image showing full deployment of the stent across the lesion, and DSA of the artery showing restored blood flow.
Angioplasty of the left superficial femoral and external iliac arteries
The same balloon was positioned at the level of the left superficial femoral artery with long inflation times. A stent mounted on an 8 X 25 balloon was positioned on the external iliac lesion relying on contour lines and imaging fusion. A closure system was put in place with a manual compression of 10 minutes.
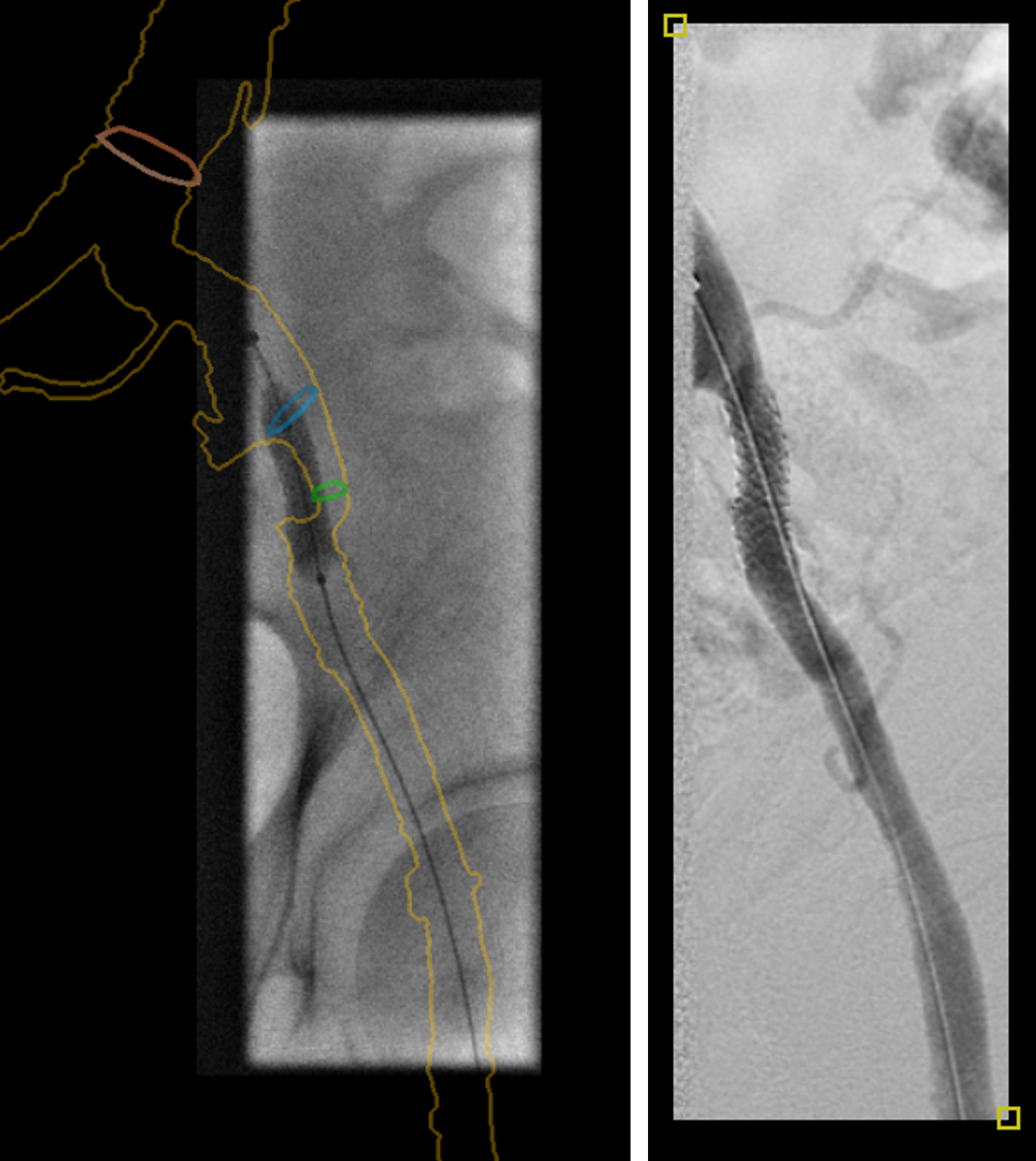
Fig 6. Balloon angioplasty and stent deployment with Vessel ASSIST image fusion in the left superficial femoral artery.
Conclusion
Complete re-opening of left lower limb was performed in the hybrid room with Vessel ASSIST. Immediate assessment with DSA showed good restoration of the blood flow in the SFA and popliteal artery. Image fusion helped detect dissections during the procedure, and thus use an appropriate catheter/ guide to cross the lesion, avoiding to use a re-entry system. Patient was discharged one day after the procedure.
Dose Levels:
|
Fluoroscopy Time |
17’21 min |
|
Dose |
4.35 Gy.cm² |
|
Air Kerma |
64 mGy |
Results may vary as many variables exist, i.e. expertise, case mix, etc., and there can be no guarantee that other customers will achieve the same results.
REFERENCES
[1] Vessel ASSIST solution includes Vision 2, VesselIQ Xpress and Autobone Xpress, and requires AW workstation with Volume Viewer and Volume Viewer Innova. These applications are sold separately. Not available for sale in all regions.