Don't have an account?

The Adequacy of Anaesthesia* (AoA) concept helps clinicians deliver an individually tailored anaesthesia and may help in their goal to improve patients' outcomes, it’s made up of parameters including EntropyTM, Neuromuscular Transmission(NMT) and Surgical Pleth Index (SPI)
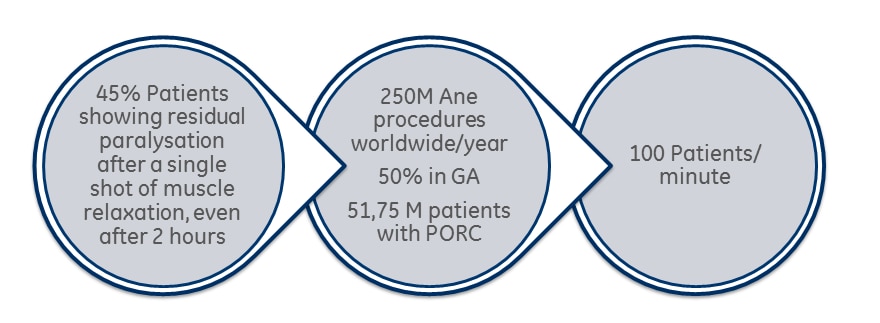
Adequacy of Anaesthesia (AoA) is a concept made up of various parameters to help clinicians assess patients' individual responses to the delivery of inhaled and intravenous hypnotics, opioids, and NMBAs during general anaesthesia.
Learn more about AoA perioperative outcomes.
The AoA concept was designed to address the different components required for general anaesthesia. Indeed, AoA parameters provide continuous non-invasive measurement of:
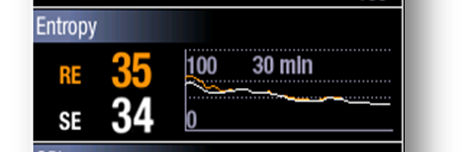
- The state of the brain with SPECTRAL ENTROPY™
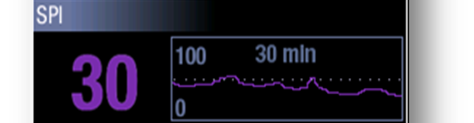
- Patient's response to surgical stimuli and analgesic medications with SURGICAL PLETH INDEX (SPI)™
- Muscle relaxation/recovery with NEUROMUSCULAR TRANSMISSION (NMT)