It can be difficult for anesthesiologists to determine the appropriate drug dosing for their patients. By utilizing both Entropy and Neuromuscular Transmission (NMT), together with other vital signs may help clinicians deliver individually tailored anesthesia and may help in their goal to improve patient outcomes. When used with monitored parameters, Entropy and NMT modules help give a more complete picture of a patient's status—all on one screen.<!-- It can be difficult for anesthesiologists to determine the appropriate drug dosing for their patients. By utilizing both Entropy and Neuromuscular Transmission (NMT), The Adequacy of Anesthesia concept together with other vital signs may help clinicians. When used with monitored parameters, Entropy and NMT modules help give a more complete picture of a patient's status—all on one screen.

According to the NAP5 report, the incidence of Accidental Awareness during General Anaesthesia (AAGA) is ~1:8,000 when neuromuscular blockade was used. They are associated with psychological consequences for the patients experiencing them, as 51% of episodes led to distress and 41% to longer-term psychological harm.1
In order to help prevent such episodes, in particular when neuromuscular blockade is used or in patients who are judged to have high risk of AAGA for other reasons, the use of depth of anaesthesia monitoring, such as Entropy monitoring, is recommended.2
For more publications, check the Entropy Publications Reference List and Entropy quick guide.
Check out Entropy Accessories
4. NAP5 Report, September 2014
5.Depth of anaesthesia monitors, NICE diagnostics guidance [DG6], November 2012
6.Vakkuri A. et al. Spectral Entropy Monitoring Is Associated with Reduced Propofol Use and Faster Emergence in Propofol-Nitrous Oxide-Alfentanil Anaesthesia Anesthesiology 2005; 103:274-9.
-->

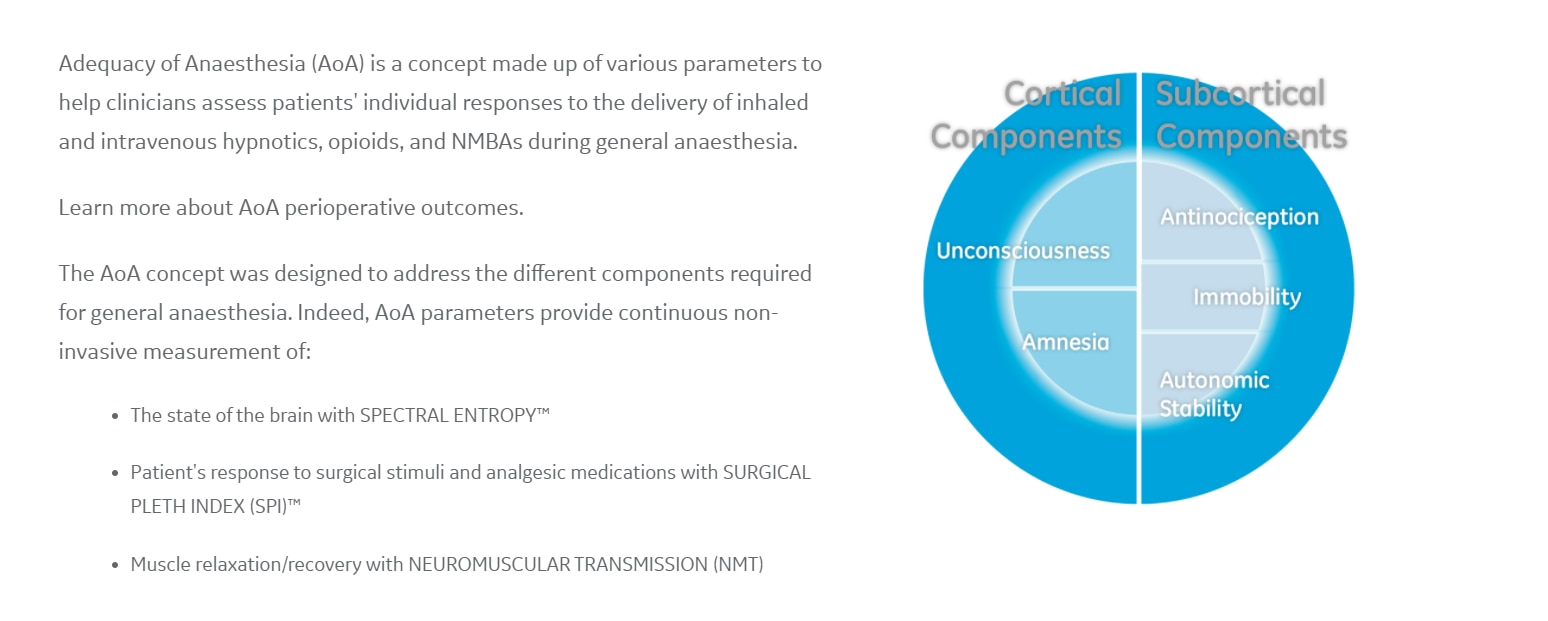

 Fig X.
Fig X.
